¶ Key Understanding:
- Reproduction is a characteristic of all living things and it is necessary for the survival of a species over time
- Poor management of one’s reproductive capabilities may lead to undesirable consequences on self and society
- Developments in science and technology have given humans greater control over their reproductive choices
- Reproduction is a characteristic of all living things
- It is the process of producing new organisms/offspring to ensure the continuity of a species.
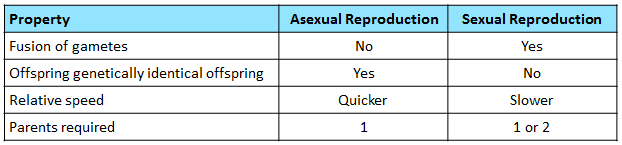
- Sexual reproduction is the process of producing genetically dissimilar offspring involving fertilisation, i.e. the fusion of the nuclei of an ovum and a sperm to form a zygote
- Is possible with one parent in hermaphrodites (bisexual organisms) which contain both types of gametes (e.g. Flowering plants)
- Is the process resulting in the production of genetically identical offspring from one parent, without the fusion of gametes
- The offspring produced are called clones>
¶ What advantages do sexual reproduction have over asexual reproduction and vice versa?
- It all depends on the environment
- Variation allows species to survive in changing environment conditions, so that they are better adapted to new environments, leading to evolution
- As clones allow species to survive in stable environment conditions, its faster mode of reproduction allows the organism to quickly populate favorable habitats
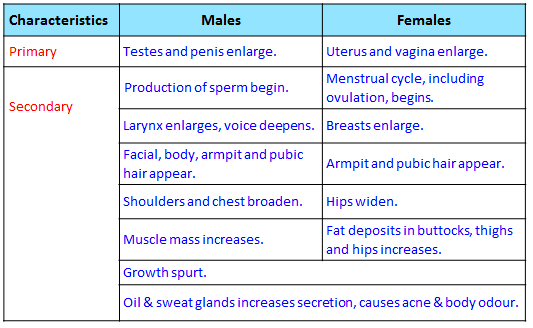
¶ Describe the physical changes during puberty and early adolescence in females and males, and classify these changes into primary and secondary sexual characteristics
- Puberty is a period of rapid growth and development
- Caused by increased secretions of sex hormones (testosterone, oestrogen & progesterone)
- To prepare the body for sexual reproduction
- Primary sexual characteristics refer to the organs in the reproductive system that are involved in sexual reproduction and are present at birth
- Secondary sexual characteristics refer to physical characteristics that develops at puberty and distinguish one sex from another, but are not directly involved in reproduction
- The physical characteristics in this definition refer to macroscopic body structures such as beard, facial hair, broad shoulders, etc. and not to sperm and ovum cells
- Hence, the scientific community disagrees on whether production of sperm and onset of menstruation should be considered a primary or secondary sexual characteristic
- As teachers and students, we are in no position to re-define biological terms; Hence although we know that the definitions are not perfect as they are a work in progress, we will take the position of Cambridge that production of sperm and onset of menstruation to be secondary sexual characteristics
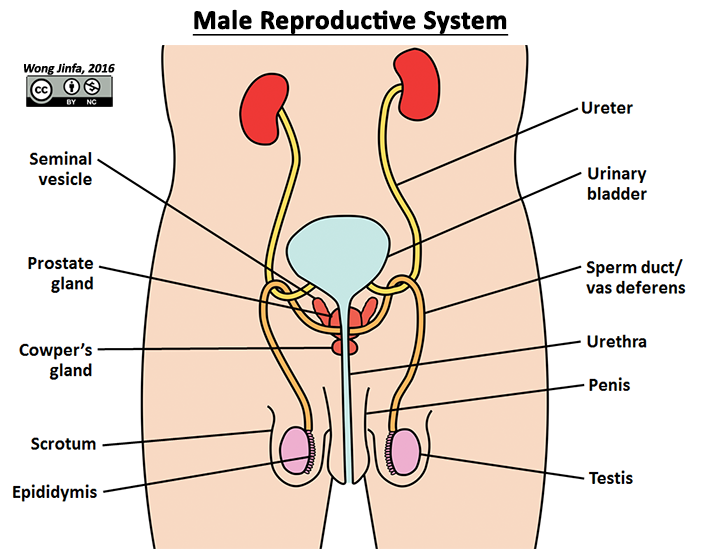
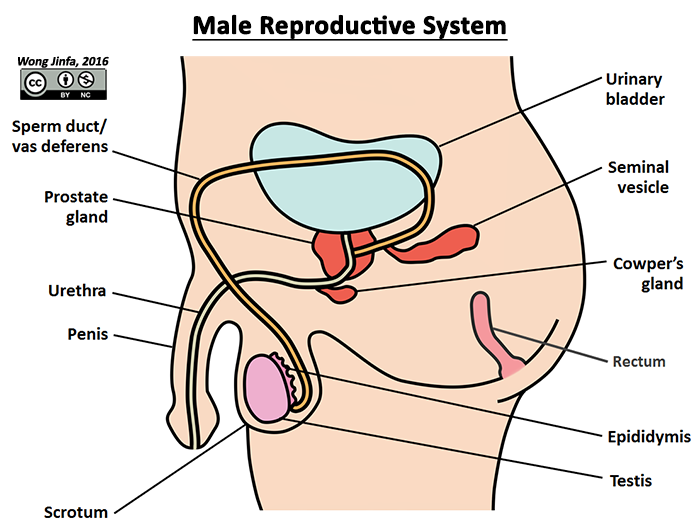
¶ Identify on diagrams, parts of the male reproductive system and describe the functions of: testis, scrotum, epididymis, vas deferens (sperm duct), prostate gland, urethra and penis
- Male sex organ that produces sperm (male gamete) and testosterone (male sex hormone)
- Stores sperm and allows them to mature
- Holds testes outside the body to maintain a lower temperature for optimum sperm development (35 to 36°C)
- Transports mature sperm to the urethra during ejaculation
¶ Prostate gland, Seminal vesicles & Cowper's gland
- Produces seminal fluid (a fluid that mixes with sperm to form semen)
- The fluid promotes survival of sperm and provides medium for sperm to swim in slightly alkaline (pH 7.2 - 8.0) to neutralize acidic environment of vagina
- Nutrient rich fluid (fructose and glucose) to provide energy for sperm to swim
- Zinc stabilizes DNA strands in sperm cells
- Mucus lubricates vagina to increase sperm mobility
- Proteins (albumin & free amino acids) for antimicrobial functions
- Transports either semen or urine out of the body, one at a single time (Sphincter muscle control opening of bladder into urethra)
- Site where semen is produced (sperm mixes with the seminal fluid produced by the prostate gland, seminal vesicles and Cowper's gland here)
- Erectile organ that fills with blood during arousal
- Enters vagina when erect to deposit semen
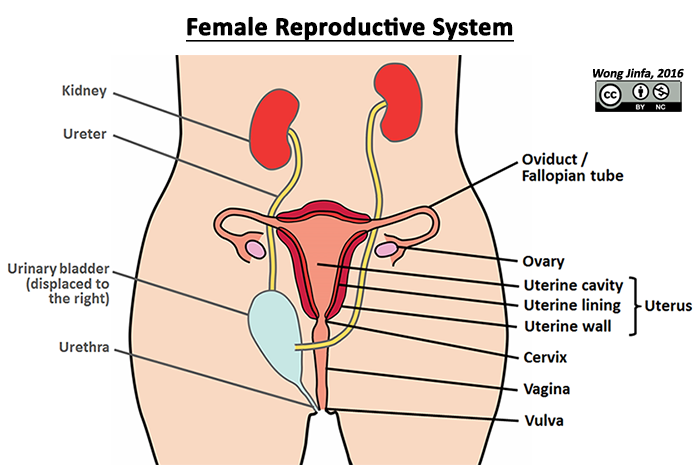
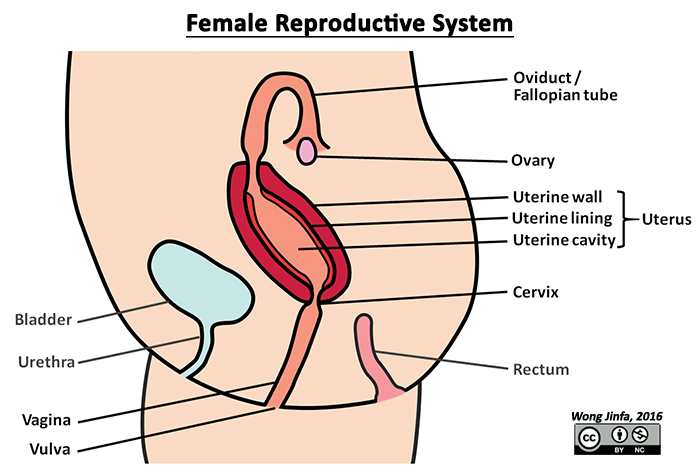
¶ Identify on diagrams, parts of the female reproductive system and describe the functions of: ovary, oviduct (Fallopian tube), uterus, cervix and vagina
- Female sex organ that produces ovum (female gamete) and oestrogen & progesterone (female sex hormone)
- One ovary releases one mature ovum (ovulation) into the oviduct every menstrual cycle
- Oviducts transport the immobile ovum down to the uterus by the action of cilia and peristaltic contractions
- Fertilisation occurs in the oviduct
- A hollow, pear shaped organ where the fetus develops during gestation
- The fertilised ovum is implanted in the endometrium (uterine lining), which is richly supplied with blood vessels during the menstrual cycle
- The uterine cavity holds the amniotic sac where fetus develops during gestation
- The smooth muscles of the uterine wall contracts during childbirth to expel the fetus
- Cervix is the narrow neck of the uterus, which dilates during childbirth
- Glands lining the cervix produce mucus
- The birth canal where sperm are deposited during sexual intercourse
- Blood and uterine tissue leave the vagina during menstruation
- Microorganisms in vagina maintains an acidic pH
¶ Describe the menstrual cycle with reference to the alternation of menstruation and ovulation, the natural variation in its length, the fertile and infertile phases of the cycle and the roles of progesterone and oestrogen only
- The main function of the menstrual cycle is to prepare the uterus to receive a fertilised ovum
- The events in this cycle are controlled by the female hormones oestrogen and progesterone
- Oestrogen is secreted by primary and Graafian follicle which thickens the uterine lining
- Progesterone is secreted by corpus luteum and maintains the uterine lining
- Menstruation (period), the monthly discharge of blood and uterine tissue through the vagina, begins the menstrual cycle
- Average length of menstrual cycle: 28 days
- Can vary between 21 – 35 days naturally
- Influenced by environmental factors
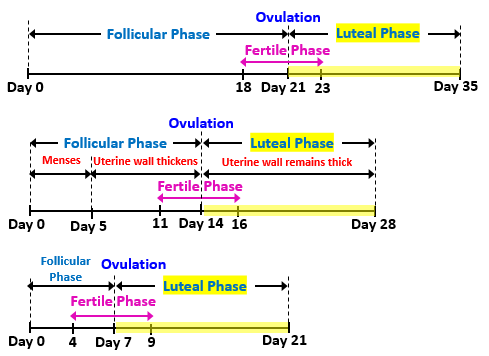
- Menstrual Flow Phase (≈ Day 1 to 5):
- Uterine lining breaks down if fertilisation did not occur
- Proliferative Phase (≈ Day 6 to 14):
- Uterine lining thickens and becomes rich in blood vessels
- Caused by an increase in oestrogen levels
- Secretory Phase (≈ Day 15 to 28):
- Uterine lining continues to thicken and maintains its thickness
- Uterine lining secretes a fluid rich in glycogen
- Caused by an increase in progesterone levels
- If a blastocyst has not been implanted in the uterine lining by the end of the secretory phase, a new menstrual flow phase begins, which marks day 1 of the next cycle
- Follicular Phase (≈ Day 1 to 14):
- Many primary follicles in the ovary begin to develop (triggered by FSH)
- Only one matures to become the Graafian follicle while the other follicles degenerate
- The follicles produce oestrogen which thicken the uterine lining
- This phase ends with ovulation, when the Graafian follicle ruptures and releases a mature ovum into the oviducts (triggered by LH)
- Luteal Phase (≈ Day 15 to 28):
- After ovulation, the Graafian follicle becomes the corpus luteum, which produces progesterone and a moderate amount of oestrogen that maintains and slightly thickens the uterine lining
- If no fertilisation occurs, corpus luteum degenerates and stops producing progesterone, causing the uterine lining to break down and the menstrual cycle begins again
- The days just before & after ovulation when a female is able to get pregnant (≈ Day 11 to 16)
- Sperm can survive up to 3 days (Ovulation day - 3 days)
- Ovum can survive up to 2 days (Ovulation day + 2 days)
- Ovulation can be detected by:
- A rise in in basal body temperature (0.4-0.8°C)
- Cervical mucus turning from white and sticky to clear, slippery and stretchy
- Calendar: 14 days from the start of menses (luteal phase is always constant)
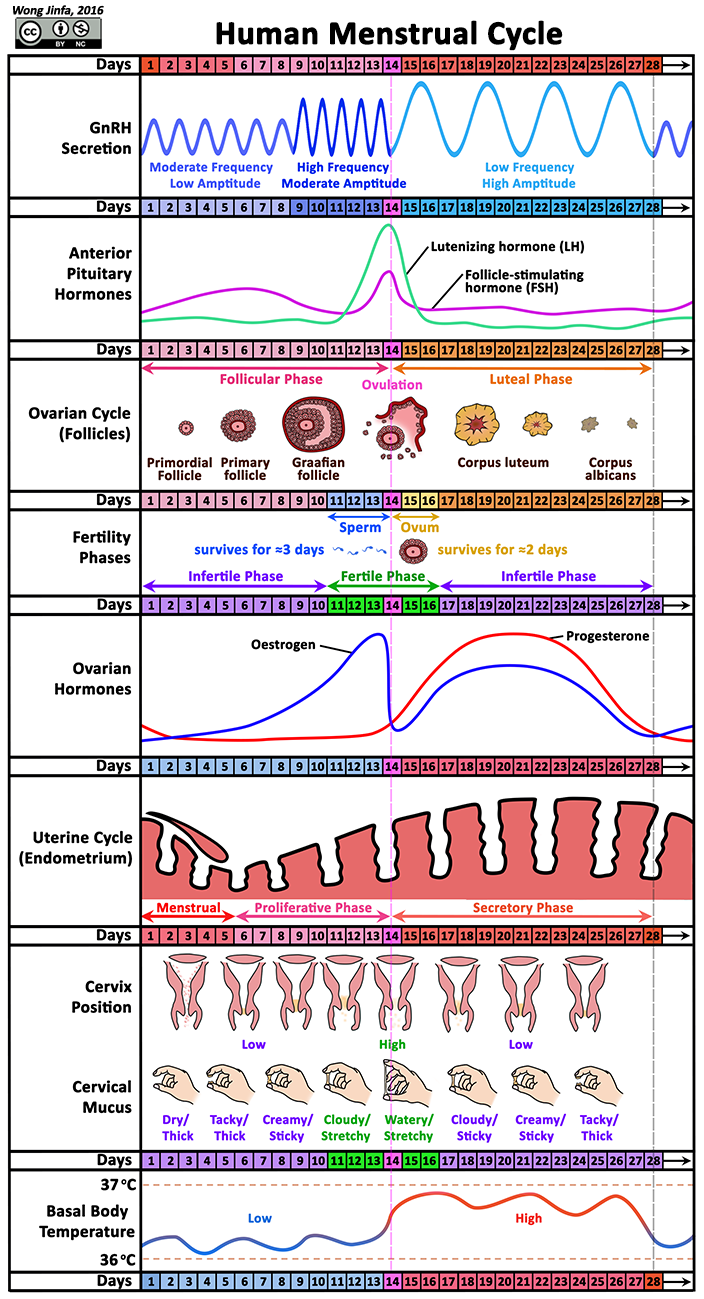
¶ Describe the roles of follicle-stimulating hormone (FSH) and luteinising hormone (LH) in the menstrual cycle
- Regulation of Female Reproductive Hormones
- Follicle-stimulating hormone (FSH) and luteinising hormone (LH) are secreted by the anterior pituitary gland when there are high levels of gondadotrophin-releasing hormone (GnRH) released from the hypothalamus (region in the brain)
- FSH stimulates the development of follicles which subsequently results in an increase in oestrogen production
- As oestrogen level increases, FSH is inhibited (negative feedback) while more LH continues to be secreted
- A peak in LH levels result in ovulation (release of the mature ovum from the Graafian follicle) and creation of the corpus luteum
- The corpus luteum secretes progesterone and oestrogen which leads to a decrease in levels of GnRH being released from the hypothalamus (negative feedback)
- The decrease levels of GnRH result in the decreased levels of FSH and LH until the end of the menstrual cycle before the cycle repeats
¶ Describe the structure of the ovum and sperm and relate its structure to its function
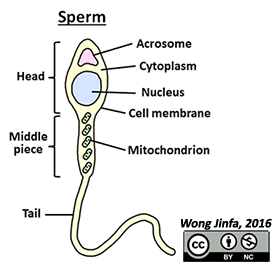
- Sperm production begins in the testes at puberty until death
- 200-500 million sperm are released in an ejaculation
- Sperm consists of three regions:
- Head which contains:
- Nucleus with half the chromosomes of a typical somatic cell (haploid)
- Acrosome which contains enzymes to penetrate the outer membrane of the ovum
- Middle piece which contains:
- Large amount of mitochondria to provide energy for swimming
- Tail / Flagellum
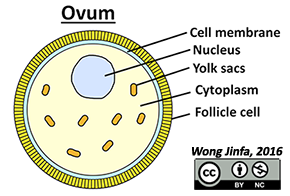
- Present in the ovaries of a female at birth (Immature ova, follicles, are present in ovaries of a female fetus)
- Released into the oviducts from the time a female reaches puberty until she reaches menopause (45-55 years old)
- At puberty, there are ≈ 400,000 follicles, but only ≈ 500 ova will be released until menopause
- Ovum is surrounded by jelly coat and follicle cells
- Large amount of cytoplasm contains nutritious yolk sacs
- Nucleus with half the chromosomes of a typical somatic cell (haploid)
¶ Describe fertilisation and development of the zygote into a ball of cells which becomes implanted in the uterine lining
- Occurs when the sperm nucleus fuses with the ovum nucleus in the oviducts
- For this to happen, the sperm has to penetrate the ovum
- When the sperm makes contact with the ovum, the sperm’s acrosome releases an enzyme that disperses the follicle cells and breaks down part of the egg membranes to allow the sperm to enter
- Only one sperm nucleus enters the ovum and fuses with the ovum nucleus, to form a zygote (a fertilised egg)
- Upon becoming a zygote, a chemical reaction alters the jelly coat composition to prevent entry of other sperm
- The sperms that were unable to fertilise the egg eventually die
- The zygote is pushed by cilia and peristalsis of the oviduct towards the uterus
- As it moves, it divides by mitosis to form a ball of cells (blastocyst)
- It typically takes the blastocyst five days to reach the uterus
- The blastocyst may float freely in the uterus for two days before it gets implanted into the uterine lining
- Implantation refers to the event where the blastocyst becomes embedded in the uterine lining
- It typically takes the blastocyst 5-7 days to implant into the uterine lining after fertilisation

- (cc) Wikipedia Ttrue12
- After implantation, some cells of the blastocyst develop into the placenta, umbilical cord and amniotic sac
- Finger-like called villi grow from the embryo into the uterine lining
- The embryonic villi and the uterine lining make up the placenta
- The placenta connects the fetus to the uterine wall via the umbilical cord, and allows exchange of nutrients, waste products, gases and antibodies
- The amniotic sac is the membrane that encloses the embryo in a fluid-filled space called the amniotic cavity
- The fluid in this cavity is called the amniotic fluid, which supports and protects the fetus
- Beautiful Images from fertilization to development of the fetus in this link.
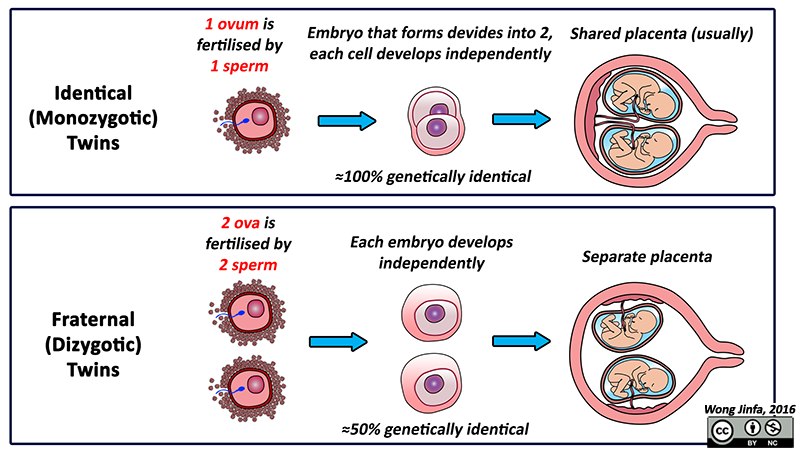
- Twins can be either identical (monozygotic) or fraternal (dizygotic)
- Identical twins are a result of the development from one zygote (monozygotic)which has subsequently divided into two
- If the time of cleavage (division) of the blastocyst is too late (≈ Days 13 to 15 after fertilisation), the twins which are born are conjoined
- Fraternal twins are a result of the development of two independent zygotes (dizygotic)
¶ Describe the function of the amniotic sac and amniotic fluid
- Amniotic sac consists of a pair of membranes, chorion & amnion

- (cc) Suparna Sinha
- Supports & allows fetus to move freely
- Protects fetus from mechanical shock
- Lubricates vagina during childbirth
- Maintains a steady internal environment for the fetus
¶ Describe the function of the placenta and umbilical cord in the exchange of dissolved nutrients, gases and excretory products between the mother and fetus
- Allows for exchange of materials between the mother and fetus by diffusion and active transport
- Without their blood mixing (as maternal and fetal blood may be of incompatible blood groups which will agglutinate if they are in contact)
- More efficiently without killing the fetus (as maternal blood is at a higher pressure and speed)
- Amino acids, fatty acids, salts, glucose, antibodies and water move from the placenta to the fetus via the umbilical vein
- Urea and other wastes are passed from the fetus to the placenta via the umbilical artery
- Acts as a barrier to prevent certain disease-causing organisms, hormones and chemicals although the protection is not complete
- Secretes hormones
- Oestrogen and progesterone to maintain the uterine lining
- Human chorionic gonadotropin maintains the corpus luteum in first trimester (Wk 1 to 12), until sufficient oestrogen & progesterone can be secreted by placenta

- (cc) OpenStax College
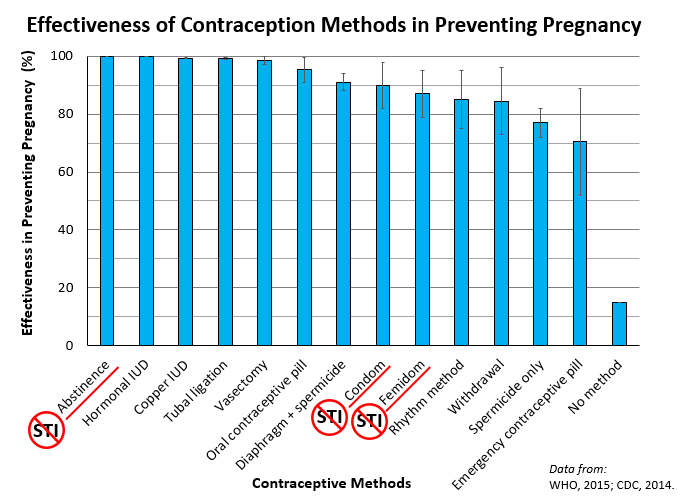
¶ Outline how various birth control methods (natural, chemical/mechanical, intrauterine devices, hormonal, sterilisation) prevent fertilisation or implantation, and/or disrupt the functions of certain organs in the reproductive system
- Contraceptives (methods to prevent pregnancy) works by preventing ovulation, fertilisation and/or implantation of blastocyst
- Contraceptives allows for family planning, allowing the prevention of overpopulation
- Contraceptives can be classified into:
- Natural
- Abstinence
- Withdrawal of penis
- Rhythm method
- Barrier
- Chemical
- Intrauterine device:
- Hormonal
- Oral contraceptive pill
- Emergency contraceptive pill
- Surgical
- Vasectomy for males
- Tubal ligation for females
- A choice to refrain from sexual intercourse and/or sexual contact
- Prevents sperm form entering the vagina and thus preventing fertilisation
- Advantages:
- Free
- No hormonal or medical side effects
- Highest (100%) success in preventing pregnancy
- Refraining from all forms of sexual contact gives the best protection against sexually transmitted infections (STIs)
- Disadvantages:
- Pressure from partner and/or peers to have sex
- The man removes his penis out of the vagina during sexual intercourse and ejaculates outside the vagina away from the female's external genitalia
- Prevents sperm from entering the vagina and thus preventing fertilisation
- Effectiveness depends on the man's ability to withdraw before ejaculation
- Pre-ejaculate may also contain sperm that can result in pregnancy
- If semen or pre-ejaculate enters the vulva accidentally, pregnancy is also possible
- Advantages:
- Free
- No hormonal or medical side effects
- Disadvantages:
- Lower (73 to 96%) success in preventing pregnancy
- Does not protect against STIs
- Requires a lot of willpower and experience (timing of withdrawal is often difficult to determine)
- When a couple avoids having unprotected sex during the fertile phase of the female's menstrual cycle
- The lady track's her fertile period by tracking her menstrual cycle, body temperature and cervical position and mucus
- Prevents fertilisation as the sperm will not meet an ovum during the infertile phases
- Advantages:
- Free
- No hormonal or medical side effects
- Disadvantages:
- Lower (75 to 91%) success in preventing pregnancy
- Does not protect against STIs
- Lady has to track her menstrual cycle daily
- Difficult to adhere to, requires discipline and cooperation from both partners
- Not very reliable as women's ovulation can be affected by anxiety, stress or illness
- Thin rubber tube that covers erect penis before sexual intercourse
- Small teat at the tip collects semen
- Forms a barrier to prevents sperm from entering the vagina as it can't pass through the rubber and thus prevents fertilisation
- Regarding usage with spermicide
- Concurrent usage with spermicide was thought to improve effectiveness to prevent fertilisation
- However, it was found that spermicides would irritate the mucosal membranes of the vagina and cervix, which increased the chance of STI transmission
- In addition, there was no evidence that spermicide lubricated condoms are better than silicone lubricated condoms, thus they should not be promoted over the other
- Advantages:
- Protects against STIs
- Can be easily obtained, relatively cheap ($1) and does not require a prescription
- Moderate (82 to 98%) success in preventing pregnancy
- No hormonal side effects
- Reversible and simple to use
- Disadvantages:
- Single use
- Sexual intercourse is interrupted as the man has to stop to put on the condom
- Some people are allergic to latex. Polyurethane condoms can be used as an alternative
- May break if it was not put on properly
- May slip off if the penis loses its erection
- Plastic (polyurethane) sheath with two flexible rings that is put into the vagina before sexual intercourse
- The smaller ring (with the closed end) is inserted into the vagina and covers the cervix
- The penis is inserted through the outer ring which remains outside the vagina
- Forms a barrier to prevents sperm from entering the vagina as it can't pass through the plastic and thus prevents fertilisation
- Advantages:
- Protects against STIs
- Can be easily obtained, relatively cheap ($4) and does not require a prescription
- Moderate (79 to 95%) success in preventing pregnancy
- Stays in place regardless of whether or not a man maintains his erection
- No hormonal side effects
- Reversible and simple to use
- Can be inserted hours before sexual intercourse
- Disadvantages:
- Single use
- Some people are allergic to the plastic
- The man needs to make sure he is inserting his penis through the ring and not at the side of the ring into the vagina
- Dome shaped rubber/silicone cap with elastic rim that is placed over the cervix to cover it
- More effective when used with spermicide
- Forms a barrier to prevents sperm from entering the cervix as it can't pass through the material and thus prevents fertilisation
- Advantages:
- Reusable (last up to 2 years)
- Relatively cheap ($15 to $75)
- Moderate (88 to 94%) success in preventing pregnancy
- No hormonal side effects
- Can be inserted 2-3 hours before sexual intercourse
- Reversible
- Disadvantages:
- Does not protect against STI
- Must be initially fitted by clinicians and purchased with a prescription
- Needs to be left inside the vagina for eight hours after sexual intercourse before being removed
- May cause serious bacterial infections if left inside the vagina for too long
- May be difficult for some women to insert
- May be dislodged before or during sexual intercourse
- Chemical in foam, cream, jelly, film, suppository or tablet form
- Chemical inactivates or kills sperm, preventing them from meeting the ovum and thus prevents fertilisation
- Usually used with other barrier methods
- Advantages:
- Can be easily obtained, relatively cheap ($8) and does not require a prescription
- Simple and easy to use
- No hormonal side effects
- Reversible
- Disadvantages:
- Low (72 to 82%) success in preventing pregnancy and hence usually used with other barrier methods
- May irritate the vagina or penis (and hence increase risk of STIs, however, changing brands may fix the problem)
- Does not protect against STIs
- Frequent use can induce lesions and ulcerations to genital mucosa lining
- Some spermicides may leak or be messy
- Small "T-shaped" device (copper wires wound around a plastic frame) that is inserted into the uterus
- Copper ions are released from the device which inactivates or kills sperm and hence prevent fertilisation
- Device also acts as a emergency contraception that prevents implantation of the blastocyst
- Advantages:
- High (99%) success in preventing pregnancy
- No hormonal side effects
- Cost can be lower in the long run compared to other birth control methods that must be purchased more frequently
- Effective for 10 to 12 years
- Does not interfere with sexual intercourse
- Reversible
- Disadvantages:
- Does not protect against STIs
- Has to be inserted by a medical professional
- May be dislodged (expulsion)
- Increases risk of infections (pelvic inflammatory disease), ectopic pregnancies and sterility
- Menstrual cramps may increase
- Irregular bleeding may occur
- Periods may be heavier and last longer (may result in anemia)
- Small "T-shaped" device that is inserted into the uterus
- Synthetic progesterone (levonorgestrel) are released from the device which:
- Alters the uterine fluid which inactivates or kills sperms and hence prevent fertilisation
- Thickens cervical mucus to prevents sperm from passing through the cervix and hence prevent fertilisation
- Leads to the thinning of the endometrial lining and hence prevents implantation of the blastocyst
- Advantages:
- High (99%) success in preventing pregnancy
- Cost can be lower in the long run compared to other birth control methods that must be purchased more frequently
- Effective for 3 to 5 years
- Does not interfere with sexual intercourse
- Reversible
- Disadvantages:
- Does not protect against STIs
- Has to be inserted by a medical professional
- May be dislodged (expulsion)
- Increases risk of infections (pelvic inflammatory disease), ectopic pregnancies and sterility
- Reduce menstrual cramps and bleeding
- May cause hormonal side effects
- Medication containing synthetic progesterone or with combination of synthetic oestrogen
- Synthetic progesterone:
- Thickens cervical mucus to prevents sperm from passing through the cervix and hence prevent fertilisation
- Leads to the thinning of the endometrial lining and hence prevents implantation of the blastocyst
- Prevents ovulation
- High levels of progesterone leads to decreased level of gonadotropin-releasing hormone (GnRH) being released by the hypothalamous, which decreases secretion of follicle-stimulating hormone (FSH) by the anterior pituitary gland
- Decreased level of FSH inhibits follicular development and decreases oesterogen production
- Lack of oestrogen results in a decrease in luteinising hormone (LH) being secreted by the pituitary gland, which prevents ovulation (that is triggered by a rapid increase in levels of LH)
- Synthetic oestrogen complements progesterone by:
- Preventing ovulation
- Inhibiting secretion of FSH by the anterior pituitary gland, which inhibits follicular development and hence prevent ovulation
- The pills are taken daily (21 pills + 7 placebo pills) or with 7 days of no pills
- Women will experience withdrawal bleeding (not menses) during the 7 days when she does not take the pill or when she is taking the placebo pill
- Advantages:
- High (91 to 99%) success in preventing pregnancy
- Makes bleeding more regular and less severe
- Regulates the menstrual cycle
- Decreases menstrual cramps, acne, risk of pelvic inflammatory disease, oesteoporosis and ovarian & endometrial cancer
- Reversible
- Disadvantages:
- Does not protect against STIs
- Needs to be prescribed by a doctor
- Has to be taken everyday or it will not be effective
- Expensive in the long run ($15 to $50 every month)
- May cause hormonal side effects
- Medication containing synthetic progesterone hormone, levonorgestrel, or with combination with synthetic oestrogen
- It is taken as an emergency method of preventing pregnancy after unprotected sexual intercourse (and should not be relied on as a birth control method)
- Works the same as an oral contraceptive pill with a higher dosage of synthetic progesterone:
- Prevents ovulation, causes cervical mucus to thicken and thins the endometrial lining
- Does not disrupt an already existing pregnancy
- Advantages:
- Relatively inexpensive ($10 to $77) and does not require a prescription
- Disadvantages:
- Low (52 to 89%) success in preventing pregnancy
- Does not protect against STIs
- May cause hormonal side effects
- Surgical procedure to permanently sterilize the man where the sperm ducts are cut and tied to prevent sperm from traveling through
- Prevents fertilisation as the man's ejaculate will not contain sperm
- The testes still continue to produce sperm but is unable to flow through the sperm duct
- The man is still able to ejaculate and have an erection
- There is a 3 months delay in taking effect where stored sperm is still present
- Advantages:
- Permanent protection against pregnancy
- High (97 to 99%) success in preventing pregnancy
- No interference with normal bodily functions or lasting side effects
- Disadvantages:
- Does not protect against STIs
- Relatively expensive ($350 to $1000) and requires a surgical procedure
- The effects are permanent and cannot be reversed
- Possible complications during surgery
- Surgical procedure to permanently sterilize the woman where the oviducts are cut and tied to prevent the ova from traveling through
- Prevents fertilisation as the sperm is unable to travel up to meet the ova in the oviducts
- Ovulation and menstrual cycle still occurs normally
- Advantages
- Permanent protection against pregnancy
- High (99%) success in preventing pregnancy
- No interference with normal bodily functions or lasting side effects
- Disadvantages:
- Does not protect against STIs
- Relatively expensive ($1500 to $6000) and requires a surgical procedure
- The effects are permanent and cannot be reversed
- Possible complications during surgery
¶ Describe the causes, symptoms, treatments, means of transmission and prevention of sexually transmitted infections (STIs) such as syphilis, gonorrhea, and HIV/AIDS
- Infections transmitted through sexual intercourse
- A person may be infected, yet shows no signs and symptoms associated with the disease
- Are caused by:
- Bacteria - e.g. Chlamydia, Gonorrhoea, Syphilis
- Virus - e.g. Herpes, HIV, Genital warts
- Fungus - e.g. Candidiasis
- Parasites - e.g. Pubic lice
- Spread through contact with an infected person's
- Body fluids - e.g. Semen, blood, vagina secretions, saliva, pus
- Mucosal membranes (Layer of epithelial cells and cells underneath it) - e.g. head of penis, vagina, rectum, eye, mouth, nostrils
- Spread by:
- Unprotected sex
- Sharing needles
- Transmission from infected mother to fetus
- Blood transfusion from infected person
- Spread of STI is reduced by:
- Abstinence
- Using condoms
- Having only one sexual partner
- Go for regular medical checkups if you are sexually active
- Asking about sexual history or requesting medical checkup of partner before sexual intercourse
- Caused by /Treponema pallidum /bacteria
- Treatment with antibiotics is effective only in the first two stages
- Can be passed from mother to child during pregnancy or childbirth, resulting in congenital syphilis
- Baby will have Hutchinson’s teeth, rashes, saddle nose
- Stage 1 (3-90 days after exposure)
- A painless sore known as chancre appears where bacteria entered the body (genitals, lips or mouth) and disappears after a few weeks
- Swollen lymph nodes around area of infection
- Symptoms may not be present
- Stage 2 (4-10 weeks after Stage 1)
- Non-itchy body rashes appear, which disappears after a few weeks
- Rash may develop into lesions, which harbor bacteria and are infectious
- Other symptoms: Fever, sore throat & weight loss
- Latent stage
- No symptoms for 10-20 years
- Non-cancerous tumor growths over the body.
- Attacks on central nervous system: Paralysis, meningitis, dementia, insanity, death
- Attacks on cardiovascular system: Heart failure
- Not infectious at this stage
- Caused by Neisseria gonorrhoeae bacteria
- Treatable with antibiotics if detected early
- Congenital gonorrhoea passes mother to child during childbirth (can't pass through placenta)
- Infects eyes, may cause blindness if not treated.
- Symptoms
- Pus discharge from penis or vagina
- Painful burning sensation during urination in men
- Lower abdominal pain, pain during intercourse in women
- If not treated, inflammation may spread to other reproductive organs, leading to
- Pelvic inflammatory disease in women
- Swollen penis, testes & prostate gland, urethritis in men
- Sterility
- Half of men and women do not show the symptoms
- Caused by human immunodeficiency virus (HIV)
- Origins have been traced to hunters who ate infected chimpanzees from Western Africa
- HIV life cycle
- Envelope glycoproteins enable virus to bind to specific receptors on certain white blood cells
- After binding, the virus fuses with the cell’s plasma membrane
- The capsid proteins contains 2 identical single-stranded RNA & 2 molecules of enzyme reverse transcriptase which are released
- Reverse transcriptase catalyses the synthesis of a DNA strand complementary to the viral RNA
- Reverse transcriptase catalyses the synthesis of a second DNA strand complementary to the first viral DNA
- The double stranded DNA is incorporated as a provirus into the cell’s DNA
- Proviral genes undergo transcription into RNA molecules, which serve as mRNA for translation into HIV proteins and genomes for the next viral generation
- Capsids are assembled around viral genome and reverse transcriptase molecules
- The new viruses bud off the host cell
- HIV infects T-cells (white blood cells/lymphocytes) of the body’s immune system and kills them
- When the body’s T-cells level fall below a certain threshold (< 200/mm3), immune system is compromised & body becomes susceptible to opportunistic infections = Full blown AIDS (cf. Healthy person: 800-1200 CD4+ T-cells per mm3 of blood)
- A person with HIV may show no symptoms for up to 10 years while T-cell counts are steadily falling
- Signs & Symptoms
- Prolonged fatigue and fever
- Swollen lymph nodes
- Chronic diarrhoea
- Unexplained weight loss
- Kaposi’s sarcoma (10-20%) - Cancer that causes patches of abnormal tissue to grow under the skin
- Lymphoma (16%) - Blood cell tumours
- Cervical cancer
- There is no cure for AIDS!
- Anti-viral drugs can only slow down progression of HIV in causing full blown AIDS
- They contain reverse transcriptase inhibitors and protease inhibitors
¶ News Articles & Videos
- Social:
- Reputation ruined or become popular
- Relationship with parents and community
- Emotional:
- Feelings of regret and guilt
- Loss of self-esteem and self-respect
- Feeling used and hurt
- Physical:
- STI transmission
- Unplanned pregnancy
- Legal:
- Abortion
- Is the removal of the embryo or fetus from the uterus before it is able to survive on its own
- Miscarriage (Spontaneous Abortion)
- Natural death of the embryo/fetus (< 20 weeks)
- Occurs in 15-30% of pregnancy; 80% in 1st trimester
- Stillbirth
- Death of the fetus in utero (after 20 weeks) or during delivery
- Premature birth
- Delivery of a live-born baby before 37 weeks
- Reasons
- Personal
- e.g. Not ready to have children, lack of financial support, too young, rape, etc.
- Health effects on mother
- e.g. Cancer, high blood pressure (pre-eclampsia), severe infection, heart failure
- Health effects on unborn baby
- Genetic abnormalities
- Multiple pregnancies
- Impending miscarriage or stillbirth
- High chance of disability or death after birth
- Abortion Procedures
- Abortifacient drugs
- Combination drug: RU-486 (Mifepristone) & Misoprostol
- RU-486 (Mifepristone) blocks progesterone which is needed to maintain the uterine lining, preventing implantation and pregnancy
- Misoprostol is take two days later which induces contractions, that expels the embryo and uterine lining
- More effective than surgical methods at early stages
- Manual or Electric Vacuumsuction aspiration
- Amniotic fluid, placenta and fetus is suctioned out from the uterus
- Dilation & Curettage (D&C)
- Dilation – Opening of the cervix.
- Curettage – Scraping of the uterine wall with a curette
- Dilation & Evacuation (D&E)
- Evacuation – Removal with surgical tools (body parts of the fetus are pulled out with a toothed clamp)
- Intact Dilation & Extraction (IDX)
- Extraction – The fetus' entire body except the head is delivered, followed by suction of the brain tissues & collapse of the skull, following full delivery
- Intrauterine instillation (saline, urea)
- Amniotic fluid is removed from the amniotic cavity and replaced with a hypertonic salt solution to kill the fetus and induce premature labour
- Dangers of abortion
- If performed safely, low risk of mother dying ~ 0.7 per 100,000 procedures in the US (Raymond /et al./, 2014)
- Minor bleeding and cramps a few days after
- Risks increases the later the pregnancy
- Unsafe abortions are performed in countries where abortion is illegal, or in developing countries
- Conducted by unskilled individuals, in unsanitary environment, or use of hazardous equipment
- Also includes self-induced abortions
- Greatly increases risk of maternal injury & death
- Health risks of abortion
- Haemorrhage
- Damage to cervix and uterus e.g. lacerations, perforations
- Incomplete removal resulting in inflammation of uterus, requiring second operation
- Pelvic inflammatory disease
- There are also emotional and psychological effects
- Relief, regret, anger, guilt, shame, emotional deadening
- Sense of loneliness, denial/memory repression, depression, insomnia, suicidal thoughts, eating disorders, difficulty maintaining relationships, drug/alcohol use, sexual dysfunction
- Abortion in Singapore
- No need for parental consent below 21
- Prohibited after 24 weeks unless mother’s life is in danger
- Mandatory counselling followed by 48 hrs wait before procedure
- Costs $600-$2000, depending on hospital
- 8515 cases in 2014, lowest in 30 years
- Rights of fetus
- Viability: When is the earliest a fetus can survive outside the womb?
- Limit of viability: Gestational age where there is a 50% survival chance of fetus outside mother’s uterus ≈ 24 weeks
- Earliest survival recorded: 21 weeks, 5 days
- Consciousness: When is the earliest a fetus can feel pain?
- The neuroanatomical system for pain (which is necessary but not sufficient for pain experience) can be considered to be completely developed by 26 weeks' gestation
- Pain experience requires development of the brain but also requires development of the mind to accommodate the subjectivity of pain
- Development of the mind occurs outside the womb through the actions of the infant and mutual adjustment through interactions with primary caregivers
- Electroencephalography suggests the capacity for functional pain perception in premature infants probably does not exist before 29 or 30 weeks
- The withdrawal reflexes and changes in heart rates and hormone levels in response to invasive procedures are reflexes that do not indicate fetal pain
- Personhood: When is the earliest a fetus is considered a person?
- First appearance of lower (week 7) or higher (week 23) brain function
- Rights of Mother
- Control over her life - e.g. Career, standard of living, relationships, emotions
- Control over her own body - e.g. Choice to have sex, health, physical appearance, limited access to contraception
- Mothers who cannot make their own decisions - e.g. Comatose, mentally disabled, mentally ill mothers
- Other Ethical Considerations
- Maximum benefit and minimum harm
- Interests of society versus rights of individual
- Autonomy versus Freedom of choice
- Justice and fairness
- Moral Arguments
- ‘Killing is wrong’ – Duty to do the right thing
- Fetus has the potential to be a human
- Should not take the risk if we are uncertain about the rights of fetus
- Religion
¶ Outline the processes involved in in-vitro fertilisation (IVF), intracytoplasmic sperm injection (ICSI), intrauterine insemination (IUI) and surrogacy and explain how these methods overcome specific causes of infertility
- Defined as inability to conceive after a year of regular unprotected (without use of contraception) intercourse
- The World Health Organisation (WHO) expects infertility and sterility to be the third most serious diseases worldwide in the 21st century, after cancer & cardiovascular diseases
- Older Age results in a decrease in quality and quantity of gametes
- Being overweightunderweight results in low sperm count in males and higher risk of infertility in females
- Unhealthy lifestyles (lack of exercise, tobacco smoking, alcohol drinking) increases risk of infertility
- Frequent strenuous intense exercise can lead to ovulation problems
- Heavy workloads, stress, environmental pollution increases risk of infertility
- Male
- Abnormal sperm productionfunction – Low sperm count and motility
- Ejaculation issues – Erectile dysfunction, premature ejaculation etc.
- Blockagedamage to male reproductive system
- Female
- Ovulation disorders
- Blockagedamage to female reproductive system
- Endometriosis (which occurs when endometrial tissue grows outside of the uterus, that release toxins that may affect the ovum)
- Uterine conditions affecting implantation and formation of the placentaamniotic sac
- General term referring to methods used to achieve pregnancy by artificial or partially artificial means
- It is used primarily in infertility treatments
- Technique in which fertilization occurs outside the womb (In vitro)
- (1) Ovarian stimulation
- Fertility drugs used to stimulate the ovaries to release multiple ova (superovulation)
- FSH (Follicular Stimulating Hormone) given over 8-14 days to stimulate the development of multiple follicles
- Multiple ova needed as some will not develop normally after retrieval
- Increase chances of pregnancy
- After 34-36 hours, and just before ovulation, ova are retrieved
- (2) Ova retrieval
- Transvaginal ultrasound aspiration
- Minor surgical procedure with anaesthesia
- Ultrasound probe inserted into vagina to identify mature follicles in the ovary
- Needle guided through vagina, into follicles
- Ova are aspirated from follicles through the needle connected to a suction device
- Laparoscopy (an instrument somewhat like a miniature telescope with a fiber optic system which brings light into the abdomen) may be used too to view the ova
- (3) Insemination & Fertilization
- Sperm obtained by ejaculation are separated from semen
- Motile sperm placed together with the ova in the process of artificial insemination
- Culture placed in incubator
- Fertilization takes place within hours after insemination
- (4) Embryo culture
- Zygote is left overnight to develop into a ball of cells (blastocyst)
- (5) Embryo transfer
- Embryos may be transferred to the uterus on either day 3 or 5 of development (blastocyst)
- One or more embryos suspended in a drop of culture medium are drawn in to a transfer catheter
- Tip of transfer catheter passed through the cervix
- Fluid with embryo placed into the uterus cavity
- Implantation will take place 2-5 days to 1-3 days after a day 3 or day 5 transfer respectively
- Helps to overcome:
- Low sperm quantity as sperm is concentrated before mixing with the ovum in the Petri dish
- Low sperm quality as only healthy sperm can be filtered out for fertilisation through a procedure known as washing
- Viscous cervical mucus as the sperm does not need to pass through it to fertilise the ovum as it is done in the Petri dish
- Blocked oviducts that prevents sperm from meeting the ovum as the sperm meets the ovum in the Petri dish
- Ovulation disorders as ovulation is stimulated through hormonal injections
- Endometriosis as the ovum is extracted directly from the ovary so it will not be affected by toxins
- Performed when rates of fertilization in IVF are poor
- Instead of mixing sperm in a culture disk, a single sperm is injected directly into an ovum
- Recommended when the male partner has a very low quality or quantity of sperm
- Increases chance greatly for fertilisation to occur but defeats the natural selection process for the healthiest sperm
- Sperm is artificially placed in the uterus with the help of a catheter
- Helps to ensure that more sperm are available and able to access a woman’s ovum
- Occur in 4 locations:
- Vagina (Intravaginal insemination or IVI)
- Cervix (Intracervical insemination or ICI)
- Uterus (Intrauterine insemination or IUI)
- Fallopian tubes (Intratubal insemination or ITI)
- Intratubal insemination is rarely used as it involves an invasive procedure
- Intrauterine insemination
- Is the most commonly used method
- Helps to overcome:
- Low sperm quantity as sperm is concentrated before insemination
- Low sperm quality as only healthy sperm can be filtered out for insemination
- Ejaculation issues as sperm will be collected, concentrated and washed before insemination into female reproductive tract
- Viscous cervical mucus as the sperm does not need to pass through it as sperm is inseminated into the uterus
- Blocked oviducts that prevents sperm from meeting the ovum as the sperm meets the ovum in the Petri dish
- Ovulation disorders as ovulation is stimulated through hormonal injections
- Sperm & egg (ovum) donors undergo extensive medical and genetic screening, including testing for AIDS
- Healthy, viable gametes will be frozen and quarantined for 6 months in the sperm bank or egg bank
- The gametes will be released to recipients only if all tests are negative
- Helps to overcome:
- Low sperm quantity and quality as sperm is obtained from the donor
- Ovulation disorders as ovum is obtained from the donor
- The practice by which a woman (called a surrogate mother) becomes pregnant and gives birth to a baby in order to give it to someone who cannot have children
- The surrogate mother is called the gestational carrier
- Gestational surrogacy
- Ovum from mother is fertilised by sperm from father through IVF except that zygote is inserted into the surrogate mother’s uterus for development
- Baby is related to both parents
- Helps to overcome issues with implantation and the same problems solved by IVF
- Traditional Surrogacy
- Ovum from surrogate mother is fertilised by sperm from father through ART
- Surrogate mother is the egg donor
- Baby is related to father but not to mother
- Helps to overcome uterine disorders in addition to the same problems solved by the ART used
¶ Discuss advantages and disadvantages of assisted reproductive technology (ART)
- Helps patients who would otherwise be unable to conceive
- Can help single women and same-sex couples
- Help to diagnose fertilisation problems
- Unused embryos can be donated to research or another couple
- Can be used to screen for inherited disease
- May be associated with side effects
- Multiple pregnancy
- Higher chance of ectopic pregnancy
- and premature birth
- Expensive
- Stressful
- Ethical issues:
- Respect for human life (when does it begin?)
- Increase in chromosomal and other congenital defects (Natural selection can’t take place?)
- Objection to playing God
- Fate of frozen embryos
- Selling of gametes, commercial surrogacy
- Lam, P. K. & E. Y. K., Lee (2013). GCE 'O' Level Biology Matters- Textbook- 2nd Edition. Marshall Cavendish Education, 463 pp.
- Hoh, Y. K. (2002). Longman A-Level Biology: Growth, Development and Reproduction. Pearson Education South Asia, 154 pp.
- World Health Organization (2015). Family Planning/Contraception. Retrieved on 11 Sep 16 from http://who.int/mediacentre/factsheets/fs351en
- Planned Parenthood (2016). Birth Control. Retrieved on 11 Sep 16 from https://www.plannedparenthood.org/learn/birth-control
- Palo Alto Medical Foundation (2015). Retrieved on 11 Sep 16 from http://www.pamf.org/teen/sexbirthcontrol
- World Health Organization (2016). Microbicides. Retrieved on 30 Oct 16 from
http://www.who.int/hiv/topics/microbicides/microbicidesen
- Niruthisard, S., Roddy, R. E., & Chutivongse, S. (1991). The effects of frequent nonoxynol-9 use on the vaginal and cervical mucosa. Sexually transmitted diseases, 18(3), 176-179. Retrieved on 30 Oct 16 from
http://journals.lww.com/stdjournal/Citation/1991/07000/The_Effects_of_Frequent_Nonoxynol_9_Use_on_the.10.aspx